 At the playground the other weekend, my 3-year-old and a couple of “big kids" were running around and climbing on everything, as you might expect. Then, out of nowhere, one of the big kids, maybe 7 years old, came flying off the “bridge” right at me. He landed from the 4-foot drop just next to me with a big, proud smile, and looked up and said: “I not scared of hypes.”
Off he ran. I smiled at his use of “hypes” for heights. The joy of words and kids! But, I was also happy at how proud he was and that he was willing to show it (not to mention he had already been kind to my daughter, which, of course, made me like him immediately!). I was curious about the fact that, while this young man wasn’t scared of heights, he knew, for some reason, it was worth telling me. He knew the concept: that being “scared of heights” is “a thing.” So, some adult had clearly introduced it, but it didn’t bother him. And, he was proud of that fact! Did he know somehow that I am scared of heights? Did he know that I am also scared I will pass this along to my daughters? Was he showing me that it was possible to talk about it, but not pass it on? Looking deeper, however, I realized this wasn’t the prompt for reflection this young man was offering at all. Heights…yeah…maybe… …but, what about hypes!? What about a fear of hypes? Is that “a thing”? Social hype? Political hype? Media hype? The list of hypes goes on and on… It turns out that, as a father, I am scared of hypes! How do I keep my daughters from internalizing a hyped-up social, political, media-driven culture of fear? Of violence? Of more…more…more? Of never good enough? Of self loathing? Of manufactured beauty? Of fake “reality”? Of real fakeness? How do I instill the tools to resist such self-destroying bombast when its sales and promotion attempt to consume them at every turn, trying to convert them into consumers of it? Somehow, I must teach my daughters to look critically at media hyperbole and its political and economic beneficiaries. They must understand there is something more than endless escalation of conflict, whether interpersonal or international, fiction, “reality,” or reality. They must see beyond the false images of self and need and desire and womanhood they will be sold when I’m not looking. How do I arm them with the nonviolent weapons of an independent mind? A critical eye on the world? A loving eye on themselves? Will they learn that they can find no peace in their world without first finding peace in themselves? Every day, this feels like the heaviest burden and greatest opportunity of being a parent. So, as a father, for my girls, hypes scare the shit out of me! But, for now, I have to just love and hope and work like hell that maybe someday my daughters, standing high, high (like crazy high!) upon a precipice (seriously, right at the edge!), grounded firmly in who they are, looking out over the beauty of the world, feeling its reflection deep within will say: I’m not scared of hypes.
0 Comments
I have written previously about hospitals thinking of physicians as customers. While it is not a perfect match, there is something important to be learned from the approach. With that in mind, I was reading recently about the Kano Model of customer satisfaction, and believe it provides a framework for understanding strategic investments in physician satisfaction and engagement. While the model is layered, in its basic form (summarized in the image below) it asks: 1. What are the “must-have” features when it comes to physician expectations of your hospital? These are also considered threshold features. And, no matter how much of a must-have feature is added, satisfaction never rises above neutral. 2. What are the “the-more-the-better” features of your hospital? These are linear features. And, as the name suggests, physician satisfaction is correlated linearly with the quantity of the feature. 3. What are the “delighter” features of your hospital? These are the features that provide the greatest satisfaction and differentiate you as a premium place to work, or to do work, for physicians. But, the lack of a delighter will never decrease physician satisfaction below neutral. 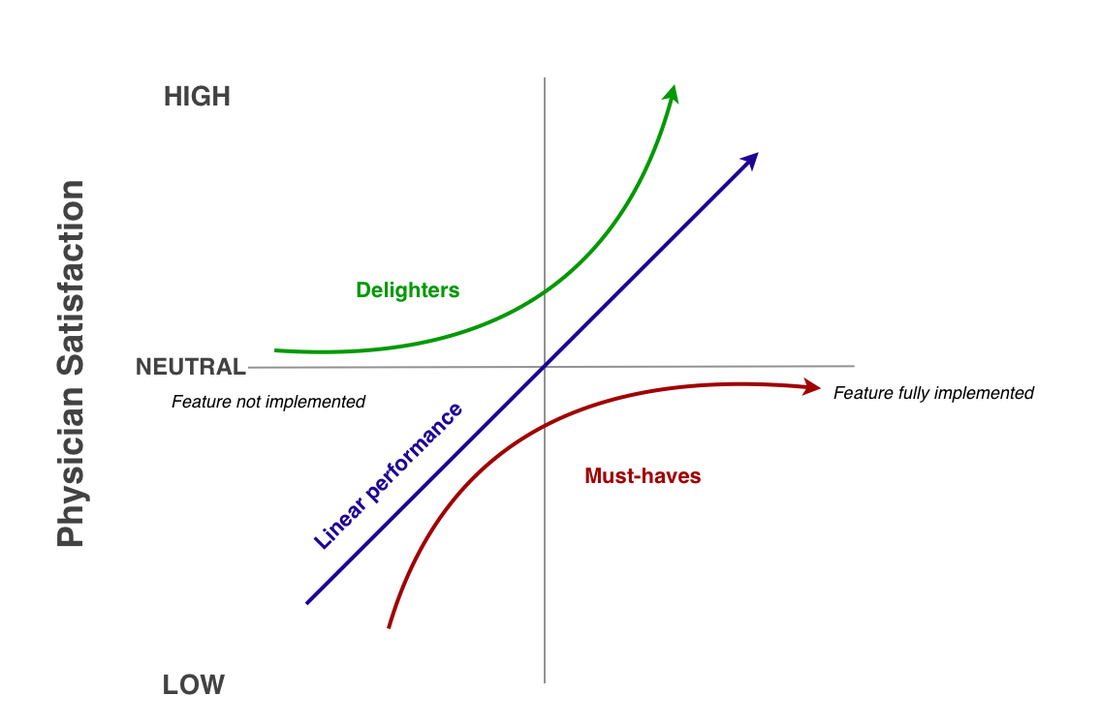 1. What do you need physicians to know?
This is about business strategy. For you to lead a safe, productive, successful hospital, what do your physicians need to know from you, or about the hospital more generally? What information is going to help align and engage physicians with the vision and direction of your hospital? What will make the hospital safer, with healthier and happier patients? When you think about hospital – physician communication, this question is fundamental. 2. What do physicians want to know? Knowing what physicians want to know and delivering it is crucial to physician engagement. It’s about professional respect. Do physicians care about hearing from the CEO or CMO? Do they want updates on policy changes and healthcare reform? Do they care about overall performance of the hospital? Are they looking for CME opportunities? Strategic internal communication has to be two-way and engage the wants and needs of both hospitals and physicians. 3. What do physicians want/need you to know? To reiterate, communication is two-way, not just in the nature and value of the content exchanged but also in who gets to initiate it. It’s about listening as much as it is about talking, posting, sending, and faxing. So, at your hospital, who gets to share information? Request information? Seek/give feedback? Report on or provide updates on hospital successes? Challenges? Who listens? Physicians need avenues to communicate with hospital leadership, to know they have been heard, and to know it matters. If they are going to engage in the vision and mission of your hospital, then they have to have a role in leading it. 4. What are you willing to change? Poor communication leads to low physician engagement. Low engagement creates communication problems. So, something has to change. What is it? What are you willing to stop that you know isn’t working? What are you wasting time, energy, and money on (ex: email newsletters with 15 pdf attachments, faxes, posters in the lounge)? What workflows need to be evaluated? What roles and expectations must change for physician support staff? For hospital executives? For physicians? Communication both creates and is a function of staffing and workflow models. So, if you want to change communication, then you must be willing to change these. Another new channel, new FTE, or new piece of technology on top of the same old practices simply won’t do it. 5. Why does it matter? If you are going to invest in change and expend your leadership capital to do so, you need a plan to articulate and promote “why” and then capture and report on the results. Can you reduce the volume of emails to a physician? Can you eliminate technologies or practices you know aren’t working anyway? Can you reduce physician stress or frustration? Can you create new feedback channels? Can you increase physicians’ sense of connection and engagement with your hospital? Communication impacts everything you do. So, pick short-term metrics that you and your physicians value and strategically align your communication change efforts to improve them. In the mid and long terms, you can then track lagging metrics like reduced turnover, increased engagement, higher productivity, increased safety and the like. |
Categories
All
Archives
April 2024
|
 RSS Feed
RSS Feed