|
This is the first question hospital and system leaders who are struggling with physician satisfaction and engagement need to ask themselves. Really, honestly, what is your relationship…today?
And, you need to respond with more than a simple “it’s bad” or “we do great” kind of answer. You need to do more than quote annual survey results. If you believe it is important, then you need to understand it deeply. If money were disappearing from your books, you would investigate, audit, and scrutinize your accounting. You certainly wouldn’t accept vagaries or wait for the results of an annual survey! Question 2: What do you need your relationship with physicians to be? In other words, to deliver quality care, build an effective culture, and produce strong, bottom-line results, what does your relationship with your physicians need to look like? How do you satisfy them and the needs of the hospital or system simultaneously? Your relationships are either a bottleneck or a gateway to your performance. They are a part of everything you do. Question 3: What do you want your relationship with physicians to be? As a leader, you can choose to invest in relationships that are transactional and fulfill the basic requirements of your hospital or system. Or, you can invest in relationships that will help you build your hospital or system, engaging and leveraging physicians as key partners, influencers, and leaders in the work. You have to start with what you actually want. Question 4: What are you willing to invest, change? Everybody talks about physician satisfaction and engagement and how important they are to hospital performance and patient outcomes. Yet, few leaders systematically and strategically invest in them as core processes of the organization. It’s not just about physician support FTEs or whether or not physicians can text you their complaints in the middle of the night, but about philosophy and approach. It’s about investing in strong physician relationships as fundamental to how you do business. How you answer these questions will in part determine how physicians will respond to you: “When physician engagement and satisfaction are both high, physicians act as “dedicated partners,” when only engagement is high they act as “discontented colleagues,” when only satisfaction is high they act as “satisfied spectators,” and when both engagement and satisfaction are low they act as “distanced patrons” (Press Ganey). Which are your physicians?
0 Comments
The problem with public education is that there isn’t enough tension. The other problem with public education is that there’s too much tension. And, perhaps the biggest problem is that both of these are correct; and we don’t distinguish between creative tension and destructive tension. Without distinguishing between the two, we cannot intentionally build structures and relationships that create the systems our students need: systems of shared leadership, strategic risk-taking, and mutual responsibility. Systems of creative tension. Instead, we more commonly build top-down structures that generate destructive tension and bottom-up structures to avoid, relieve, or push back against them. At all levels and relationships, public education is replete with destructive tension. Whether it’s the policymaker focusing on test scores he has no control over, the School Board trying to improve classroom practice it has no experience with, or the district administrator trying to empower principals who have systematically been disempowered, we lack the structures and processes to support creative tension. So, our tension becomes destructive, structural stress, which becomes a self-fulfilling and redundant system of production. So, what are the key differences between a structure that produces destructive tension and one that generates creative tension? 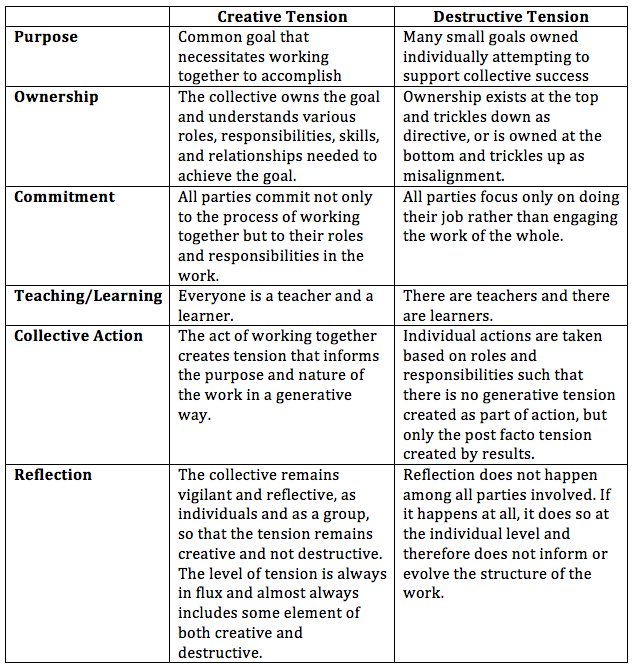 The following shows two possibilities for some relatively simply planning among school faculty to improve student outcomes. While this just illustrates the start of planning, the same models and considerations can be extended through all stages of action, reflection, assessment, and improvement.
Making a Plan: The Destructive Tension Approach A principal is approached by a group of teachers who are concerned about increased expectations to provide interventions and supports for students with intellectual disabilities, but without any additional planning time for new strategies. The principal listened to their concerns and then explained the rationale he used when making this decision. He assured them it was the right decision for their school. The principal recommended that the teachers use their current individual prep time to collaborate with other staff and develop individualized plans to meet students' needs. He asked to see their plans at the next staff meeting. Making a Plan: The Creative Tension Approach A principal is approached by a group of teachers who are concerned about increased expectations to provide interventions and supports for students with intellectual disabilities without additional time to develop and plan for the new strategies. The principal adds this topic to the agenda of a staff meeting scheduled for the next week. In that meeting, he asks staff to consider what each is doing in their classroom to ensure all learners have equitable access to instruction in meeting their individual needs. (Reflection) Through the discussion, the staff begins to recognize that too many learners are not finding success and that staff as a whole uses a fairly narrow range of interventions. (Ownership) Together with the principal, they agree on a shared goal to adopt a wider variety of interventions and supports to increase student success and identify the ones they want to focus on first. (Purpose) As part of this, they make a plan to have fellow teachers who are experts in the priority areas provide brief peer-to-peer professional development opportunities during each staff meeting. Over time, they aspire to have each teacher share their successes and challenges with the group. (Commitment, Teaching/Learning) The principal and staff develop a plan to allocate time for teachers to plan for implementation and engage a teacher coach to provide modeling and time to practice and refine their skills. (Collective Action) The principal and staff schedule regular, frequent opportunities to reflect and refine practice individually, with the coach, and in professional learning communities. (Reflection) To reduce the destructive tension that often undercuts efforts to improve how our schools function, intentional practices that nurture creative tension need to be imbedded throughout the relationships within the school and across a school system. Note: These relationships include not only adults, but also the young people as the largest stakeholder in public education. In their absence as a constituent in the variables of the creative tension model, we will never build structurally creative systems. Keep an eye out for our next blog to focus on creative tension among young people and adults. Written by: Anderson Williams, Teri Dary, and Terry Pickeral originally published by the Learning First Alliance I attended a healthcare technology event recently where a hospital CEO told the audience: “physicians are an extension of your brand.” While I liked the clarity of the statement, I felt it only represented part of the unique and complicated relationship between physicians and “the brand.”
As a hospital or a healthcare system, your physicians are more than an extension of your brand; they are consumers of it. And, this dual relationship is critical to understand as you seek to satisfy, engage, align, and whatever else you want to do in partnership with physicians to increase performance. Before they can become an extension of your brand, or at least an extension of what you want your brand to be, physicians must be treated like your consumers. So, as with any product or service, you need to effectively market who you are, what you offer, and why you align with their existing values and goals (not just hope that they align with yours). If patients are consumers of healthcare, then physicians, in many ways, are consumers of healthcare organizations. As a cultivated and dedicated consumer, a physician can become an extension of the brand you are seeking to build. (They already extend the brand: good, bad, or otherwise.) You need physicians to share your values, vision, and understand your direction. In turn, you provide the tools and supports for them to deliver on them. Physicians should feel a personal connection with the brand and other high-level leaders within the organization who represent it. Here are a few recommendations for cultivating the physician brand consumer/extension: Identify what your brand is – internally – and market it.Marketing campaigns are typically focused on reaching consumers outside of the hospital or system. For the physician consumer, however, your message is almost certainly different than the one targeting the public (albeit ideally consistent from a values perspective). If you understand and believe in the physician-as-consumer, you must commit to strong and consistent internal messaging and marketing. Connect performance and brand.Good hospital performance means a lot of things: healthy patient outcomes, positive patient experiences, increased safety, lower stress, and a strong bottom line. All of these have an impact at the individual level, but cumulatively they build a powerful brand that people at all levels want to be a part of. So, your branding internally is not about taglines, it’s about values and your collective ability to deliver on those. Communicate your brand strategically and consistently.Your communication both creates and reflects the relationships you have with your physicians. So, if it is noisy and sporadic and only tactical or transactional, that’s the kind of relationship you will build with physicians. None of us is committed to a brand, whether it’s technology, tennis shoes, or a hospital, that communicates this way. And, if you choose to, your physicians probably won’t commit to you either. |
Categories
All
Archives
April 2024
|
 RSS Feed
RSS Feed